

A long-overdue shift: What the new NICE fertility guidelines mean for people with endometriosis
Written by Sophie Sulehria

For years, people living with endometriosis have found themselves navigating not just a complex and often debilitating condition, but a fertility system that didn’t quite know where to place them.
Despite affecting an estimated 1.5 million women in the UK, endometriosis has too often sat in a grey area when it comes to fertility care - misunderstood, inconsistently managed, and, for many, minimised.
That is why the latest update from NICE - National Institute for Health and Care Excellence matters.
Because for the first time, endometriosis has been given its own dedicated section within fertility guidelines.
And that seemingly simple structural change carries significant weight.
From “unexplained” to understood
One of the most important shifts in the updated guidance is what it moves away from.
Historically, people with endometriosis have often been grouped under the umbrella of “unexplained infertility” - a category that, while clinically convenient, has long been frustrating for patients who already have a diagnosis.

During the consultation phase, organisations including Endometriosis UK raised concerns about this exact issue.
Because endometriosis is not unexplained.
It is a diagnosed, systemic condition that can impact fertility in multiple ways - from inflammation and adhesions, to ovarian function and implantation.
By recognising this and creating a distinct pathway, NICE is doing something crucial: it is validating both the condition and the experience of those living with it.
As Eric Power, Interim Director of the Centre for Guidelines at NICE, put it, patients and clinicians made it clear that endometriosis “needed its own pathway.”
This update delivers that.
Why this change matters in practice
On paper, a new section in a guideline might sound administrative.
In reality, it has the potential to reshape conversations in clinics across the country.
For patients, it signals something powerful: that their condition is recognised as a legitimate and complex factor in fertility - not something to be sidelined or simplified.
For clinicians, it provides a clearer framework for decision-making, encouraging more personalised, evidence-based discussions rather than a one-size-fits-all approach.
And perhaps most importantly, it aims to reduce the inconsistency that has long defined fertility care for people with endometriosis.
Because until now, access to treatment has often depended on where you live, who you see, and how your symptoms are interpreted.
That variability has come at a cost - emotionally, physically, and financially.
Moving beyond “mild” and “severe”
Another key shift in the guidance is the move away from simplistic labels like “mild” and “severe” endometriosis.
These terms have long been used in clinical settings, but many patients and clinicians have argued they fail to capture the reality of the condition.
Someone with so-called “mild” endometriosis can experience debilitating pain and significant fertility challenges, while others with more extensive disease may have fewer symptoms.
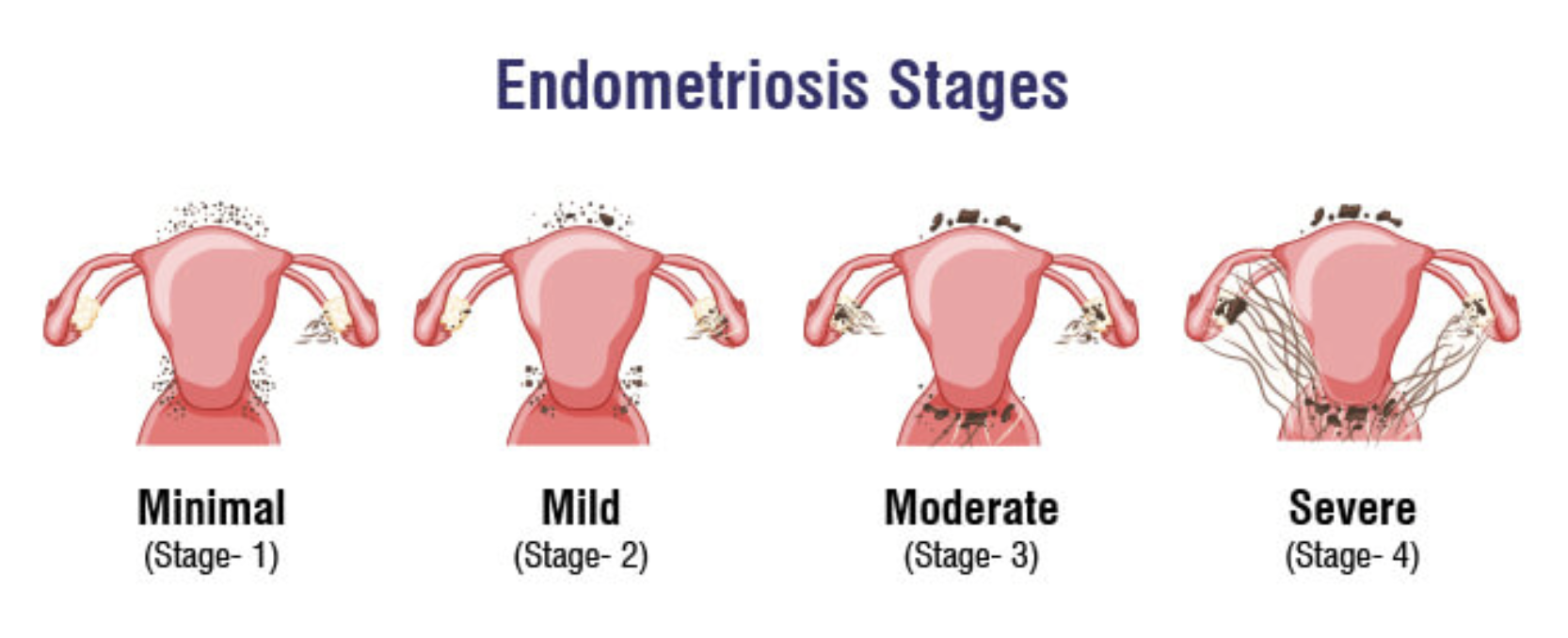
Fertility outcomes don’t always correlate neatly with staging.
By acknowledging this, NICE is encouraging a more nuanced understanding - one that reflects the complexity of the condition rather than reducing it to a label.
This matters because labels shape decisions.
And decisions shape outcomes.
A more personalised fertility pathway
At the heart of the updated guidance is a clear emphasis on individualised care.
Rather than applying rigid timelines or assumptions, clinicians are advised to consider a range of factors when supporting people with endometriosis who are trying to conceive.
These include:
How long they have been trying for a baby
Their age
The severity and nature of their symptoms
Their ovarian reserve
Any male factor fertility issues
This may sound obvious, but it marks an important shift away from blanket approaches.
Because fertility is never one-dimensional.
And when endometriosis is part of the picture, that complexity only deepens.
What does the pathway actually look like?
The guidance outlines a staged approach, offering patients options rather than a single prescribed route.
Initially, individuals may be supported to try to conceive naturally, depending on their circumstances.
For some, surgical treatment to address endometriosis may be considered - particularly where there are symptoms or anatomical factors that could be affecting fertility.
What’s important here is choice.
Patients are not funnelled into one pathway but are instead supported to make informed decisions based on their specific situation.
After up to two years of this approach, fertility treatments such as intrauterine insemination (IUI) or IVF can be discussed.
Again, this is not a rigid rule but a framework - one that aims to balance giving people time with avoiding unnecessary delays.
Because for many, time is not neutral.
Breaking down barriers to treatment
One of the strongest messages in the updated guidance is around access.
NICE has been clear that once endometriosis is diagnosed, patients should not face additional barriers when seeking fertility treatment.
This is significant.
Because historically, many people with endometriosis have reported being asked to “wait and see,” even when they already have a known condition that could impact fertility.
Others have faced delays in referral or inconsistencies in eligibility criteria across different regions.

Public Health Minister, Sharon Hodgson, described the update as a “landmark” step towards reducing these barriers and creating a clearer, more consistent pathway.
That consistency is key.
Because access to care should not depend on postcode, persistence, or luck.
The wider context: diagnosis and delay
This update doesn’t exist in isolation.
It follows earlier NICE guidance on the diagnosis and management of endometriosis, published in November last year, which aimed to speed up diagnosis and improve referral pathways.
That’s an important piece of the puzzle.
Because one of the biggest challenges with endometriosis is not just how it is treated, but how long it takes to be recognised in the first place.
On average, diagnosis can take years.
Years of pain.
Years of being told symptoms are normal.
Years of not having answers.
By the time many people reach a fertility clinic, they are already carrying that history.
So while this new guidance is a step forward, it also highlights the need for earlier recognition and intervention.
A note on testing: What not to rely on
The updated guidance also includes a caution around the use of anti-Müllerian hormone (AMH) testing.
Specifically, it warns against using AMH levels as a predictor of clinical pregnancy through spontaneous conception.
This is an important clarification.
AMH is often used as a marker of ovarian reserve - essentially, an indication of how many eggs someone may have.
But it does not tell us whether someone will get pregnant naturally.
In a landscape where fertility testing can sometimes feel overwhelming or oversimplified, this reminder matters.
It reinforces the idea that no single test can define someone’s fertility journey.
Looking beyond the obvious: coeliac disease and fertility
Another interesting addition to the guidance is the suggestion to consider serological testing for coeliac disease in people with unexplained sub-fertility.
While not directly related to endometriosis, it reflects a broader shift towards more holistic thinking in fertility care.
Because fertility is influenced by a wide range of factors - some of which may not be immediately obvious.
By encouraging clinicians to look beyond the usual pathways, NICE is opening the door to more comprehensive assessments.
What still needs to change
While this update is undoubtedly a positive step, it is not a complete solution.
Guidelines can shape practice, but they do not automatically change it.
Implementation will be key.
That means ensuring clinicians are aware of the changes, that services are equipped to deliver them, and that patients feel empowered to advocate for themselves within this new framework.
It also means addressing the broader systemic issues that continue to affect fertility care - from regional funding disparities to long waiting times.
And crucially, it means continuing to listen to patients.
Because as this update has shown, meaningful change often starts with lived experience.
A shift in tone, as much as policy
Perhaps what stands out most about this update is not just what it changes, but how it reframes the conversation.
It moves away from ambiguity and towards clarity.
Away from generalisation and towards personalisation.
Away from minimisation and towards recognition.
For people with endometriosis, that shift matters.
Because fertility is not just a clinical issue.
It is deeply emotional, often uncertain, and profoundly personal.
To be seen within that - to have your condition acknowledged, your experience validated, and your options clearly laid out - is no small thing.
The bottom line
The updated NICE fertility guidelines mark a significant step forward for people with endometriosis.
By creating a dedicated pathway, challenging outdated labels, and emphasising personalised care, they offer the potential for more consistent, compassionate, and effective support.
But as with any guideline, their impact will depend on how they are applied in practice.
For now, though, the message is clear.
Endometriosis is no longer an afterthought in fertility care.
And for the 1.5 million people in the UK living with the condition, that recognition is long overdue.